

Magnesium, along with calcium, sodium and potassium is a part of the macro-mineral family. It is purported to be the fourth most abundant mineral in the human body after calcium, sodium and potassium (Schwalfenberg and Genuis, 2017). As such, it is a key cofactor in more than three hundred (300) enzymatic functions in the body and thus is essential for the biochemical functioning of several metabolic pathways (Schwalfenberg and Genuis, 2017).
Research contends that the human body contains around twenty-five grams (25g) of magnesium (Martyka et al. 1996), of which twenty-seven percent (27%) is in the muscles, fifty-three percent (53%) in the bone and nineteen percent (19%) in the soft tissues and less than one percent (1%) in the blood serum (Fawcett, 1999; Elin, 2010).
Magnesium has been touted as having many benefits such as calming the nervous system, helping with sleep as well as strengthening the muscles of the heart. All of which have been proven by research. Magnesium can be found in foods such as broccoli, hemp seeds, spinach, pumpkin seeds, and low-fat yoghurt as well as an additive in some processed foods.
It is also available in supplement form which provides a variety of ways to add it to one’s diet to ensure that our bodies receive the required dosages of this critical nutrient. Let’s Discuss!
What is Magnesium?
Magnesium is one of those minerals that are critical to our overall health and well-being but unfortunately, can be deficient without knowing it until we start to experience particular symptoms. Even then, we may not realize it has the cause because it is not one of those deficiencies doctors readily test for.
According to research, humans are more at risk for magnesium deficiency due to the decrease in magnesium levels in food crops, the easy access to refined and processed foods, the presence of chronic diseases and even medications (J. DiNicolantonio et al., 2018). For example, processed white flour or white rice has been found to lower one’s magnesium levels by up to 300-400% J. DiNicolantonio et al. 2018).
Additionally, phytic acid which is found in foods such as nuts, grains, and seeds including hemp seeds has also been shown to diminish the absorption of magnesium (Russo and Reggiani, 2013). However, the magnesium found in food kinds, especially those in plant foods has been shown to improve one’s magnesium status (Lopez, et al. 2004).
The risk of magnesium deficiency can signify even more danger for some individuals causing them to supplement even more with magnesium to prevent magnesium deficiency.
Normal blood serum magnesium is said to be between .75 to .95 millimoles per litre (mmol/L). Any reading that is lower than that is considered low magnesium levels or a deficiency (Costello et al, 2016). However, some researchers recommend that magnesium be given to patients who are experiencing magnesium deficiency-related symptoms if the serum level is below 0.9 mmol/L (Liebscher and Liebscher, 2004).
On the other hand, serum magnesium levels that are above 0.95 mmol/L may indicate that the individual is experiencing a condition known as hypermagnesaemia. Hypermagnesaemia is a situation where too much magnesium is in the blood. This usually occurs in individuals who are suffering from renal failure or poor kidney function (DiNicolantonio et al. 2018).
Nevertheless, let us not wait until our bodies start to manifest symptoms that doctors may find difficult to diagnose or yield a prognosis of magnesium deficiency.
In this article, we will look at how having adequate magnesium in the diet can benefit the body as well as prevent the occurrence of certain diseases. As such, the article will explore how magnesium can help with quality sleep, migraine headaches, diabetes, depression as well as cardiovascular health.
Five (5) Health Benefits of Magnesium
- It may help to promote quality sleep.
- It may help with migraine headaches.
- May help to manage diabetes.
- It may help with depression.
- May help with cardiovascular health.
Magnesium and Sleep Quality
The sleep and wake cycle is regulated by the brain (Moore, 2007). As such, sleep deprivation as well as the quality of sleep has been linked to many metabolic and cardiovascular irregularities (Cappuccio, et al. 2010; Reimer and Flemons, 2003). To this extent, the quality of sleep or lack thereof has been manifested as sleep disorders such as feeling sleepy during the day, falling asleep during times when we should be awake as well as snoring during sleep (Cao, et al. 2018). Further, the foods we consume during the day can impact the quality of sleep.
For example, carbohydrate-high foods with a high glycemic index can make one feel sleepy. On the other hand, a diet low in fiber but high in saturated fats and sugar can lead to less restorative sleep as well as waking up more times during sleep (St-Onge, et al. 2016; Cao, et al. 2016; Afaghi, et. al. 2007).
Additionally, many studies have directly linked quality sleep to inadequate mineral intake (Cao et al, 2018). One such mineral, magnesium, has been found to regulate cellular timekeeping and thus aid in quality sleep both in plants and animals (Feeney, et al. 2016).
Additionally, in a double-blinded placebo-controlled study it was found that supplementing the diet with magnesium can improve symptoms of insomnia in older people (Abbasi et al. 2012), while low magnesium intake was associated with depression which the study found to be positively related to poor sleep. However, these studies were conducted with the supplementation of magnesium instead of dietary sources. As such, the research contends that the link between dietary magnesium and sleep was limited.
Nonetheless, in a five (5) year study by (Cao et al., 2018), it was found that dietary intake of magnesium-rich foods was associated with a reduced risk of falling asleep during the day in women but not particularly in men. Additionally, the study found no direct correlation between dietary magnesium intake and other sleep disorders such as insomnia or snoring during sleep in both men and women.
Magnesium and Migraine Headache
A headache is just not a headache, especially when it comes to migraines, which have been defined as severe throbbing head pain. Additionally, migraine headaches can be accompanied by eye pain, nausea or even vomiting as well as sensitivity to light or sound. These types of sensations accompanying migraines are formally called ‘an aura’ (Mayoclinic.com).
To this extent, migraine headaches are stated as being the most common form of disabling headache that afflicts approximately twelve percent (12%) of the population of Western societies (Lipton, et al. 2007).
However, while over-the-counter medication may provide partial relief; studies have shown that magnesium is a safe and effective acute treatment option for migraine relief and prevention (Yablon and Mauskop, 2011). Further, over the years, some studies have suggested that magnesium deficiency may play a role in the pathogenesis of migraine.
While most of the theories then, were not proven; subsequent research has found that patients suffering from migraine headaches were deficient in magnesium (Jain et al, 1985; Ramadan et al. 1989; Schoenen et al. 1991).
However, it has been argued that this research must be taken with an air of caution as the tissue of some of these very patients showed both normal and low levels of magnesium. As such, Altura et al., (1992) purported that the study should be based on ionized magnesium as a true indication of magnesium metabolism to truly measure the variability of the results. Ionize magnesium is the active form of total magnesium (U.S. National Library of Medicine, 2016).
The effectiveness of ionized magnesium was proven in a study measuring the level of ionized magnesium in forty (40) participants who were experiencing an acute migraine attack. The study found that half of the patients, fifty percent (50%) had really low levels of magnesium (Mauskop et al., 1995). When the patients were administered one gram (1g) of magnesium sulfate, eighty-six percent (86%) reported sustained pain relief for over a Twenty-four (24) hour period (Leao, 1944).
Additionally, in a double-blinded placebo-controlled randomized study, it was found that magnesium supplementation was associated with a significant decrease in the frequency of migraine attacks as well as severity (Koseoglu et al., 2008). It must be noted that the magnesium used in this study was magnesium citrate. The study was also extended to women suffering from menstruation-related migraine and comprised over two hundred and seventy (270) women, sixty-one (61) of whom had menstruation-related migraine.
The research showed that forty-five (45%) percent of the women were deficient in magnesium during menstrual-migraine attacks while fifteen (15%) percent experienced migraine during non-menstrual attacks (Mauskop et al. 2002). Conversely, it was also found that the ratio of calcium to magnesium levels was elevated in women during menstrual-related migraine even though these same women had normal ionized calcium levels.
Nonetheless, while many studies have found that magnesium deficiency does impact the onset of headaches including migraines others have proven otherwise. For example, a placebo-controlled double-blinded study by Pfaffenrath et al. (1996) showed no effect of magnesium on migraine. However, the researchers attributed this finding to the possible use of poorly absorbed magnesium salt.
This assumption was made because more than half of the participants complained of experiencing side effects of diarrhea. Therefore, this suggests that the relief of migraine will largely be dependent on several factors which include the quality of the magnesium chosen, the rate of absorption as well as the amount of magnesium taken.
Magnesium and Diabetes
Diabetes is a condition in which the body is unable to produce or respond to the hormone – insulin. This results in the abnormal metabolism of carbohydrates in the human body. The abnormal metabolism of carbohydrates eventually leads to elevated levels of glucose in the blood and thus Diabetes (Dictionary.com). Diabetes can be of two (2) Types – Type 1 and Type 2. When an individual has Type 1 Diabetes, then his/her body does not produce insulin (Atkinson and MacLaren, 1994).
On the other hand, an individual with type 2 diabetes, doesn’t respond to insulin but produces some level of insulin on its own (Reaven et al. 1976; Tuomilehto et al. 2001). As the disease progresses, then the body does not make enough insulin. Both type-1 and type-2 diabetes lead to high blood sugar levels over time which can cause the development of further complications in the body.
According to research, individuals with diabetes mellitus usually have a magnesium deficiency which is typically shown to be inversely related to insulin sensitivity (de Valk, 1999). As such, research shows that magnesium supplementation can improve insulin sensitivity as well as insulin secretion in individuals with type 2 diabetes. However, the study did not demonstrate any beneficial results in one’s glycaemic control with the oral supplementation of magnesium (de Valk, 1999).
Additionally, the research also showed some indication of the benefits of magnesium in lowering blood pressure. However, more research is recommended as it relates to magnesium being used as a preventive agent in the development of type 2 diabetes as well as the progression of retinopathy, a condition that affects persons with type 2 diabetes (de Valk, 1999).
To this extent, research suggests that conventional diabetes therapies, as well as oral magnesium supplementation, may delay the onset of complications of diabetes (de Valk, 1999) as well as improve insulin sensitivity and metabolic control in patients with type 2 diabetes. This was concurred in a study by Shahbah et al. (2017) on how oral magnesium can improve the glycemic control and lipid profile of children with type 1 diabetes as well as those with hypomagnesaemia.
The study confirmed an optimization of glycemic control as well as an increase in protective lipids with the supplementation of magnesium. It must be noted that the study was conducted over a three (3) month period with a magnesium intake of three hundred and fifty milligrams (350 mg) of magnesium oxide. The patients’ magnesium serum level was less than 1.7 mg/dl, which indicated a deficiency in magnesium.
Magnesium and Depression
Depression is a mood disorder which is now considered a worldwide epidemic affecting over three hundred and fifty million (350) people worldwide. It is forecast to become one of the leading causes of disease burden by the year 2030 (World Health Organization, 2012).
Depression is not a new phenomenon, as we all experience feelings of being depressed at some time or another. Some of the clinical signs of depression include a feeling of sadness and hopelessness, loss of interest, anxiety and reduced appetite among others (mayoclinic.com). However, the symptoms of depression become chronic when it is experienced over a long period and begins to affect one’s lifestyle and those around them.
The immediate treatment for depression is usually antidepressants. Nonetheless, research has shown that only fifty (50%) percent of patients realize remission (Trevino et al., 2014) while twenty (20%) percent still suffer from symptoms even after two (2) years.
To this extent, research has indicated that other methods, particularly non-pharmacologic approaches are needed. Further, while cognitive behaviour therapy and lifestyle interventions can be effective, these types of interventions require highly trained therapists as well as several months of treatment to be effective (Hoifodt et al., 2011). As such, magnesium is now being researched as a viable option in the treatment or management of depression (Jacka et al., 2009; Huang et al., 2012; Tarleton and Littenberg, 2015; Yary et al., 2016).
While magnesium is found predominantly in foods such as hemp seeds, broccoli, spinach, low-fat yoghurt, buckwheat flour etc, supplementation is still seen as a practical option, especially as it relates to the management of depression. This was highly documented in a twelve (12) weeks open-label randomized control trial of one hundred and twenty-six (126) adults suffering from mild to moderate symptoms of depression.
The participants were supplemented with magnesium chloride. As such, they all took five hundred milligrams (500 mg) tablets of magnesium chloride daily for a total of two hundred and forty-eight milligrams (248 mg) of elemental magnesium per day (Tarleton et al. 2017).
According to the researchers, magnesium chloride was chosen because it is highly absorbable and tolerable compared to some other forms of magnesium (Durlach et al., 2005; Martin et al., 1998). The results showed a change in depression symptoms as well as changes in the symptoms of anxiety. Therefore, it was concluded that magnesium was effective for the treatment of mild-to-moderate depression in adults. It was also observed that magnesium worked quickly and was well tolerated with no reported adverse reactions.
Additionally, while some trials found magnesium chloride to be effective in the treatment of depression in adults (seniors) with type 2 diabetes (Barragan-Rodriguez et al. 2008) others have shown magnesium citrate to be effective at decreasing depression in individuals with fibromyalgia (Bagis et al., 2013). As such, different forms of magnesium may yield similar or different results.
Therefore, it may be a trial-and-error sort of scenario to see which one works best for your situation and/or your body can tolerate. It is also important that you are guided by a medical professional when starting any supplementation regimen, especially in cases where another medical condition exists.
Magnesium and Cardiovascular Health
Magnesium is an essential dietary mineral that is critical to key biological processes in the human body. As such, it is important to the functioning of major organs and systems, including the cardiovascular system (Rosique-Esteban et al., 2018). The cardiovascular system or circulatory system is a system organ that allows blood to circulate and transport nutrients to the cells of the body to help fight diseases, stabilize the body’s temperature as well as maintain overall homeostasis of the body (National Council Institute; yourdictionary.com). The cardiovascular system includes the heart, blood and blood vessels (your dictionary.com.).
When the functions of the body’s system are interrupted, this can set off a slew of conditions in the body and thus, the development of diseases. Therefore, a diet rich in fruits and vegetables is necessary for the optimal and continuous proper function of the cardiovascular system. Further, when the diet is deficient in one mineral, then that too can initiate the breakdown of the enzymatic functions and of course, the occurrence of diseases (Institute of Medicine, US, 1992).
Research has shown that higher magnesium intake has a beneficial effect on the risk factors for cardiovascular diseases (Shechter, 2010). For example, high magnesium intake improves glucose and insulin metabolism as well as acts as an anti-inflammatory agent (Shechter, 2010). Further, an intake of magnesium has been shown by studies to provide protection against stroke (Larsson et al., 2012; Nie et al., 2013; Adebamowo et al., 2015).
This was concurred by Fang et al., (2016) in a study with fourteen (14) participants. In their study, they found that a dietary magnesium intake of at least one hundred milligrams per day (100 mg/day) lowers the risk by at least twenty-two percent (22%).
It must be noted that in most of these studies, magnesium intake included both dietary means and supplementation. In addition, research cautions that the consideration of other factors such as age, sex and country may help to provide more conclusive results as it relates to the effect of magnesium on cardiovascular risks (DiNicolantonio et al. 2018).
This was especially due to the common diets in particular countries. For example, in Japan, magnesium levels were reportedly below the Japanese Recommended Daily Allowance (RDA) for people between the ages of 15-49 years old (Itokawa, 2005) while over forty-eight percent (48%) of the US population reportedly consume less than the recommended amount of dietary magnesium (Rosanoff et al., 2012).
Additionally, in France, reports suggested that twenty-three percent (23%) of women and eighteen percent (18%) of men experienced inadequate magnesium intake (Vormann and Anke, 2002).
A Case for Magnesium Deficiency
According to Costella et al. (2016), it is estimated that about fifty percent (50%) of Americans do not obtain adequate amounts of magnesium daily. While no current data on magnesium status is available in Jamaica, older data purports that about 15% to 20% of the population of developing countries, suffers from magnesium deficiency (Durlach, 1989).
These data do provide some serious level of concern in the field of medical science that has attributed magnesium deficiency to the increasing epidemic of some chronic diseases (C.Lo, 2000) as well as mental health issues. Nonetheless, there remains insufficient scientific literature on the issue of magnesium deficiency as it pertains to particular health outcomes (Schwalgenberg and Genius, 2017).
The level of magnesium deficiency has been attributed to several factors such as the increase in consumption of processed food as well as the diminished levels of magnesium in foods both organic and non-organic alike (Griffiths et al., 2012).
For example, common food types such as white flour, are said to have between twenty – twenty-five milligrams of magnesium for every one hundred grams (20-25 mg/100 gm) and sugar, which is itself cited as a major concern in many studies due to its purported health risk to human has 0 mg/100 gm.
As such, these staples are said to contribute less than twenty percent (20%) of the daily recommended allowance of magnesium (Heaton, 2003). Further, how foods are prepared also reduces the level of magnesium. For example, cooking and boiling produce will result in a significant reduction in the level of magnesium (Heaton, 2003).
Additionally, a deficiency in vitamin D can also cause the body to experience difficulties in absorbing magnesium (Krejs et al., 1983) as well as certain types of medications including antibiotics, drugs for hypertension and the use of antacids (Fawcett et al. 1999; Campbell et al., 2014).
Other lifestyle habits such as alcohol intake, cigarette smoking as well as being inflicted with type 2 diabetes also affect the absorption of magnesium (Jahnen-Dechant and Ketteler, 2012). Further, as we age, the level of magnesium absorption is also reduced by at least thirty percent (30%) (Schwalgenberg and Genuis, 2017).
Some signs of Magnesium Deficiency
According to Schwalgenberg and Genuis, (2017) and DiNicolantonio et al. 2018) some of the symptoms of magnesium deficiency include:
- Cardiac changes (ECG and arrhythmias).
- Depression.
- Seizures.
- Muscle weakness.
- Muscle cramps.
- Nerve issues.
- Facial twitching.
- Confusion.
- Migraine headaches.
- Vertigo.
- Irritability.
- Aggression.
- Vitamin D resistance.
While magnesium deficiency has been proven to create many issues in the human body, an excessive amount of magnesium can also create issues, for example, bone health. As such, research has shown that excessive oral magnesium supplementation can suppress bone turnover in postmenopausal women as well as in young adult males (Aydin et al., 2010; Dimai et al., 1998).
Therefore, it’s best to stay within the recommended daily allowances unless guided otherwise by a healthcare professional.
How do you know when you have consumed too much magnesium?
One of the most common indications of too much magnesium intake is gastrointestinal issues. So, if after consuming foods high in magnesium or taking a supplement you rush to the bathroom, then you may have consumed too much. Additionally, with higher intake comes the risk of magnesium toxicity (Schwalgenberg and Genuis, 2017).
As such, lower your intake, stop altogether or see a medical professional if you experience laxative effects, diarrhea, dizziness with a drop in blood pressure, pelvic and back pain or respiratory or breathing issues and confusion.
How much magnesium should I take then?
According to the Institute of Medicine (IOM), the upper tolerable limit of magnesium supplementation with no risk of gastrointestinal side effects is 420 mg/day for men and 320 mg/day for women (Food and Nutrition Board, US). Additionally, individuals with known medical conditions such as renal impairment may be at a higher risk of adverse effects (National Academies Press, 1997; Bailey et al, 2011).
Nonetheless, before supplementing with magnesium, guidance must be sought from a medical professional if one is already suffering from known medical conditions.
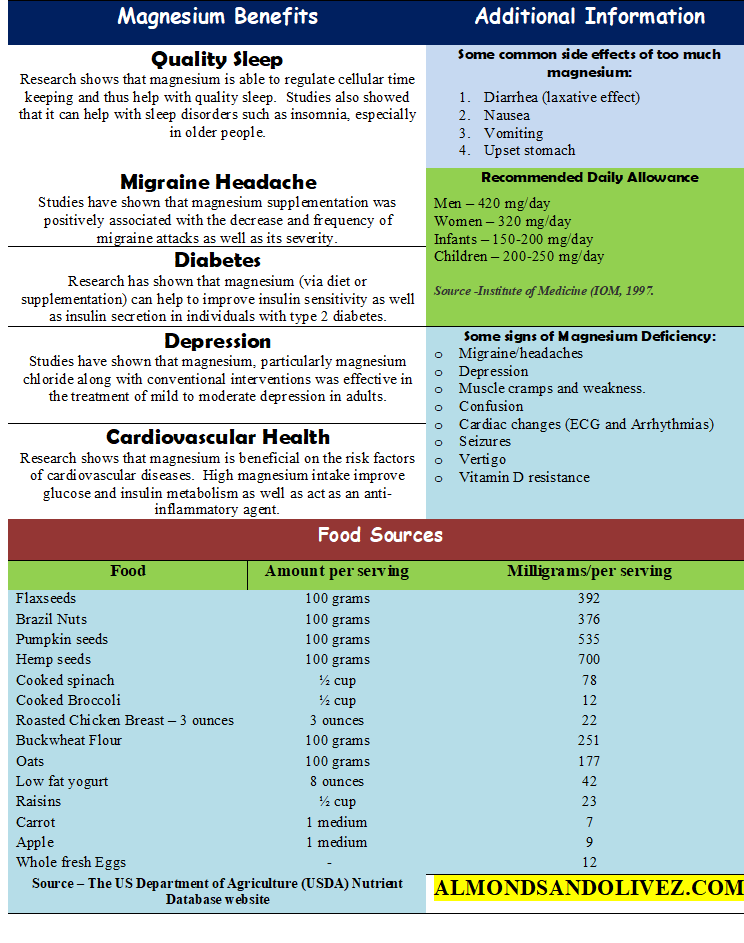
Illustrative Summary
Here is a summary of how magnesium can benefit the body as well as its food sources and side effects as well as Recommended Daily Allowance (RDA).
Let’s Sum Up!
Magnesium is an essential dietary mineral that plays a key role in the biological functions of the human body. As such, it acts as a co-factor for more than three hundred (300) enzymatic functions of the body along with other minerals such as calcium, potassium and sodium. To this extent, research has shown that deficiencies, especially up to the level of chronic are associated with the development or prolonged deterioration of certain chronic diseases including diabetes and hypertension.
In addition, research has shown that a daily intake of at least 100 mg/day can be beneficial for migraineurs (persons suffering from migraine headaches). Other benefits of magnesium include quality sleep, diabetes and cardiovascular health.
Additionally, over the years, research has shown that magnesium has been used as a viable treatment option for depression. While most studies have experimented with magnesium chloride and oxide, others have shown that the other types of oral magnesium supplementation such as citrate, sulfate etc show no inferior benefits.
Dietary sources of magnesium include broccoli, spinach, hemp seed, pumpkin seed, buckwheat flour, apple, carrot and low-fat yoghurt among others. Remember, nothing in isolation. As such, all minerals are critical to the proper function of the body.
Further, all supplementation, even in minor, must be discussed or be guided by your health care professional. So now that we have discussed the importance of this critical nutrient, what will you do differently?
You can also check out this post on another powerful ingredient here, as well as some other posts below:
- Spirulina – the ultimate guide including Five (5) scientific proven benefits.
- Elderberry – What it is and Five (5) Benefits that make it one of the world’s renowned berries!
- Pine Bark Extract and Arthritis – Is there a positive link? Let’s Explore the Research!
References and Further Reading
- Abbasi, B.; Kimiagar, M.; Sadeghniiat, K.; Shirazi, M.M.; Hedayati, M.; Rashidkhani, B. (2012). The effect of agnesium supplementation on primary insomnia in elderly: A double-blind placebo-controlled clinical trial. J. Res. Med. Sci. 17, 1161–1169.
- Adebamowo, S.N.; Spiegelman, D.; Willett, W.C.; Rexrode, K.M. Association between intakes of magnesium, potassium, and calcium and risk of stroke: 2 Cohorts of US women and updated meta-analyses. Am. J. Clin. Nutr. 2015, 101, 1269–1277.
- Afaghi, A.; O’connor, H.; Chow, C.M. (2007). High-glycemic-index carbohydrate meals shorten sleep onset. Am. J. Clin. Nutr. 85, 426–430.
- Altura BT, Shirley T, Young CC, Dell–‐Ofrano K, Handwerker SM, Altura BM (1992). A new method for the rapid determination of ionized Mg2+ in whole blood, serum and plasma. Meth Find Exp Clin Pharmacol 14:297–‐304.
- Atkinson M, Maclaren , N. (1994). The pathogenesis of insulindependent diabetes mellitus. N Engl J Med 331:1428-1436.
- Aydin, H., Deyneli, O., Yavuz, D. et al. (2010). “Short-term oral magnesium supplementation suppresses bone turnover in postmenopausal osteoporotic women,” Biological Trace Element Research, vol. 133, no. 2, pp. 136–143.
- Bagis S, Karabiber M, As I, Tamer L, Erdogan C, Atalay A. Is magnesium citrate treatment effective on
- pain, clinical parameters and functional status in patients with fibromyalgia? Rheumatol Int. 2013; 33
- (1):167±72. https://doi.org/10.1007/s00296-011-2334-8.
- Bailey, RL, Fulgoni III VL, Keast D.R, Dwyer, J.D (2011). Dietary supplement use is associated with high intakes of minerals from food sources. Am J Clin Nutr ;94:1376-81.
- Barragan-Rodriguez L, Rodriguez-Moran M, Guerrero-Romero F. Efficacy and safety of oral magnesium
- supplementation in the treatment of depression in the elderly with type 2 diabetes: a randomized,
- equivalent trial. Magnes Res. 2008; 21(4):218±23.
- Cao, Y.; Wittert, G.; Taylor, A.W.; Adams, R.; Shi, Z. (2016). Associations between Macronutrient Intake and Obstructive Sleep Apnoea as Well as Self-Reported Sleep Symptoms: Results from a Cohort of Community Dwelling Australian Men. Nutrients , 8, 207.
- Campbell, S. C. Stockmann, C. , Balch, A. et al. (2014). “Intrapartum magnesium sulfate and the potential for cardiopulmonary drug-drug interactions,” Therapeutic Drug Monitoring, vol. 36, 4, pp. 544–548.
- Cappuccio, F.P.; D’elia, L.; Strazzullo, P.; Miller, M.A. (2010). Quantity and quality of sleep and incidence of type 2 diabetes: A systematic review and meta-analysis. Diabetes Care, 33, 414–420.
- Costello, RB, Elin RJ, Rosanoff A, et al. Perspective: the case for an evidence-based reference interval for serum magnesium: The time has come. Advances in Nutrition: An International Review Journal 2016;7:977–93.
- Lo, (2000). “Integrating nutrition as a theme throughout the medical school curriculum,” American Journal of Clinical Nutrition, vol. 72, supplement 3, pp. 882S–889S.
- de Valk HW. (1999). Magnesium in diabetes mellitus. Neth J Med. 54(4):139-46.
- DiNicolantonio JJ, et al. (2018). Open Heart ;5:e000668. doi:10.1136/openhrt-2017-000668.
- Dimai, H. Porta, S. Wirnsberger, G. et al. (1998). “Daily oral magnesium supplementation suppresses bone turnover in young adult males,”The Journal of Clinical Endocrinology &Metabolism, vol. 83, no. 8, pp. 2742–2748.
- Durlach J. Recommended dietary amounts of magnesium: Mg RDA. Magnes Res 1989;2:195–203.
- Durlach J, Guiet-Bara A, Pages N, Bac P, Bara M. Magnesium chloride or magnesium sulfate: a genuine question. Magnes Res. 2005; 18(3):187±92. PMID: 16259379.
- Elin, R.J (2010). “Assessment of magnesium status for diagnosis and therapy,” Magnesium Research, vol. 23, no. 4, pp. S194–S198.
- Fang, X.; Wang, K.; Han, D.; He, X.; Wei, J.; Zhao, L.; Imam, M.U.; Ping, Z.; Li, Y.; Xu, Y.; et al. Dietary magnesium intake and the risk of cardiovascular disease, type 2 diabetes, and all-cause mortality: A dose—Response meta- analysis of prospective cohort studies. BMC Med. 2016.
- Fawcett, W. Haxby, E.J., & Male, D.A. (1999). “Magnesium: physiology and pharmacology,” British Journal of Anaesthesia, vol. 83, no. 2, pp. 302–320.
- Feeney, K.A.; Hansen, L.L.; Putker, M.; Olivares-Yañez, C.; Day, J.; Eades, L.J.; Larrondo, L.F.; Hoyle, N.P.; O’Neill, J.S.; van Ooijen, G. Daily magnesium fluxes regulate cellular timekeeping and energy balance. Nature 2016, 532, 375–379.
- Griffiths, A.M., Cook, D., Eggett, D. & Christensen, M.J. (2012). “A retail market study of organic and conventional potatoes (Solanum tuberosum): mineral content and nutritional implications,” International Journal of Food Sciences and Nutrition, vol. 63, no. 4, pp. 393–401.
- Heaton, F.W. (2003). “Magnesium metabolism and its disorders,” The Clinical Biochemist Reviews, vol. 24, no. 2, pp. 47–66.
- Hoifodt RS, Strom C, Kolstrup N, Eisemann M, Waterloo K. Effectiveness of cognitive behavioural therapy in primary health care: a review. Fam Pract. 2011; 28(5):489±504. https://doi.org/10.1093/fampra/ cmr017 PMID: 21555339.
- Huang JH, Lu YF, Cheng FC, Lee JN, Tsai LC. Correlation of magnesium intake with metabolic parameters, depression and physical activity in elderly type 2 diabetes patients: a cross-sectional study. Nutrition J. 2012; 11(1):41. https://doi.org/10.1186/1475-2891-11-41 .
- Institute of Medicine (US) Committee on Diet and Health; Woteki CE, Thomas PR, editors. Eat for Life: The Food and Nutrition Board’s Guide to Reducing Your Risk of Chronic Disease. Washington (DC): National Academies Press (US); 1992. Chapter 8, Vitamins, Minerals, And Chronic Diseases. Available from: https://www.ncbi.nlm.nih.gov/books/NBK235010/
- Itokawa Y. [Magnesium intake and cardiovascular disease]. Clin Calcium 2005;15:154–9.
- Jacka FN, Overland S, Stewart R, Tell GS, Bjelland I, Mykletun A. Association between magnesium intake and depression and anxiety in community-dwelling adults: the Hordaland Health Study. Aust N Z.
- J Psychiatry. 2009; 43(1):45±52. https://doi.org/10.1080/00048670802534408.
- Jain AC, Sethi NC, Balbar PK. (1985). A clinical electroencephalographic and trace element study with special reference to zinc, copper and magnesium in serum and cerebrospinal fluid (CSF) in cases of migraine. J Neurol Suppl 232:161.
- Jahnen-Dechent, W. & Ketteler, M. (2012). “Magnesium basics,” Clinical Kidney Journal, vol. 5, supplement 1, pp. i3–i14.
- Koseoglu E, Talashoglu A, Gonul AS, Kula M (2008). The effects of magnesium prophylaxis in migraine n without aura. Mag Res 21:101–‐8.
- Kotlinska-Hasiec, E., Makara-Studzinska, M. Czajkowski, M. et al (2017). “Plasma magnesium concentration in patients undergoing coronary artery bypass grafting,” Annals of Agricultural and Environmental Medicine, vol. 24, no. 2, pp. 181–184.
- Krejs, G. Nicar, M. Zerwekh, J.E., Norman, D.A., Kane, M.G. & Pak, C.Y. (1983). “Effect of 1,25-dihydroxyvitamin D3 on calcium and magnesium absorption in the healthy human jejunum and ileum,” The American Journal of Medicine, vol. 75, no. 6, pp. 973–976.
- Kutsal E, Aydemir C, Eldes N, Demirel F, Polat R, Taspnar O, Kulah E. Severe hypermagnesemia as a result of excessive cathartic ingestion in a child without renal failure. Pediatr Emerg Care 2007;23:570-2.
- Larsson, S.C.; Orsini, N.; Wolk, A. Dietary magnesium intake and risk of stroke: A meta-analysis of prospective studies. Am. J. Clin. Nutr. 2012, 95, 362–366.
- Leao AAP (1944). Spreading depression of activity in cerebral cortex. J Neurophysiol 7:159–390.
- Liebscher DH, Liebscher DE. (2004). About the misdiagnosis of magnesium deficiency. J Am Coll Nutr ;23:730S–1.
- Lipton, RB, Bigal, ME, Diamon, M. AMPP Advisory Group (2007). Migraine prevalence, disease burden, and the need for preventative therapy. Neurology 68:343–‐9.
- Littenberg B, MacLean C. Intra-cluster correlation coefficients in adults with diabetes in primary care practices: the Vermont Diabetes Information System field survey. BMC Med Res Methodol. 2006; 6(1):20. https://doi.org/10.1186/1471-2288-6-20.
- Lopez-Ridaura, R ., Willett, W.C., Rimm, E.B., et al., “Magnesium intake and risk of type 2 diabetes in men and women,” Diabetes Care, vol. 27, no. 1, pp. 134–140, 2004.
- Martin RW, Perry KG Jr., Martin JN Jr., Seago DP, Roberts WE, Morrison JC. Oral magnesium for tocolysis: a comparison of magnesium gluconate and enteric-coated magnesium chloride. J Miss State Med Assoc. 1998;39(5):180±2
- Martyka Z, Kotela I, Blady-Kotela A. [Clinical use of magnesium]. Przegl Lek 1996;53:155–8.
- Mauskop A, Altura BT, Cracco RQ, Altura BM (1995) Intravenous magnesium sulphate relieves migraine attacks In patients with low serum ionized magnesium levels: a pilot study. Clin Sci 89:633–‐6.
- Mauskop A, Altura BT, Altura BM. (2002). Serum ionized magnesium levels and serum ionized calcium/ionized Magnesium ratios in women with menstrual migraine. Headache 42:242–‐8.
- Moore, R.Y. (2007). Suprachiasmatic nucleus in sleep-wake regulation. Sleep Med., 8 (Suppl. 3), 27–33.
- Nie, Z.-L.; Wang, Z.-M.; Zhou, B.; Tang, Z.-P.; Wang, S.-K. Magnesium intake and incidence of stroke: Meta-analysis of cohort studies. Nutr. Metab. Cardiovasc. Dis. 2013, 23, 169–176.
- Pfaffenrath V, Wessley P, Meyer C, Isler HR, Evers S, Grotemeyer KH, Tanieri Z, Soyka D, Gobel H, Fisher M (1996) Magnesium in the prophylaxis of migraine: a double–‐bind, placebo–‐controlled study. Cephalalgia 16:436–‐40.
- Ramadan NM, Halvorsan H, Vande–‐Linde A, Levine SR, Helpern JA, Welch KMA (1989). Low brain magnesium in migraine. Headache 29:590–‐3.
- Reaven, GM, Bernstein R, Davis B, Olefsky J. Non-ketotic diabetes mellitus: Insulin deficiency or insulin resistance? Am J Med 1976; 60:80-88.
- Reimer, M.A.; Flemons,W.W. (2003). Quality of life in sleep disorders. Sleep Med. Rev. 7, 335–349.
- Romani, A. (2014). Magnesium in Health and Disease. Springer Science and Business Media Dordrecht;
- Rosanoff A, Weaver CM, Rude RK. Suboptimal magnesium status in the United States: are the health consequences underestimated? Nutr Rev 2012;70:153–64.
- Rosique-Esteban, N, Marta Guasch-Ferré , Pablo Hernández-Alonso & Jordi Salas-Salvadó .(2018). Dietary Magnesium and Cardiovascular Disease: A Review with Emphasis in Epidemiological Studies. Nutrients ,10, 168; doi:10.3390/nu10020168.
- Rude, R.K. (1992). Magnesium deficiency and diabetes mellitus. Causes and effects. Postgrad Med;92:217–24.
- Shechter, M. Magnesium and cardiovascular system. Magnes. Res. 2010, 23, 60–72.
- Schoenen J, Sianard–‐Gainko J, Lenaerts M (1991) Blood magnesium levels in migraine. Cephalalgia 11:97–‐9.
- Schwalfenberg, G.K, Genuis, S.J. The Importance of Magnesium in Clinical Healthcare. Scientifica (Cairo). 4179326. doi: 10.1155/2017/4179326. Epub 2017 Sep 28.
- Shahbah, Doaaa & Hassan, Tamer & Morsy, Saed & Saadany, Hosam & Fathy, Manar & Al-Ghobashy, Ashgan & Elsamad, Nahla & Emam, Ahmed & Elhewala, Ahmed & Ibrahim, Boshra & Gebaly, Sherief & Sayed, Hany & Ahmed, Hanan. (2017). Oral magnesium supplementation improves glycemic control and lipid profile in children with type 1 diabetes and hypomagnesaemia. Medicine. 96. e6352. 10.1097/MD.0000000000006352.
- St-Onge, M.P.; Roberts, A.; Shechter, A.; Choudhury, A.R. (2016). Fiber and Saturated Fat Are Associated with Sleep Arousals and SlowWave Sleep. J. Clin. Sleep Med. 12, 19–24.
- Tarleton, E. K., Littenberg, B., MacLean, C. D., Kennedy, A. G., & Daley, C. (2017). Role of magnesium supplementation in the treatment of depression: A randomized clinical trial. PloS one, 12(6), e0180067. doi:10.1371/journal.pone.0180067.
- Tarleton EK, Littenberg B. Magnesium intake and depression in adults. J Am Board Fam Med. 2015;2(2):249±56.https://doi.org/10.3122/jabfm.2015.02.140176.
- The National Academies Press, Dietary Reference Intakes for Calcium, Phosphorus,Magnesium, Vitamin D, and Fluoride,The National Academies Press,Washington, DC, USA, 1997.
- Trevino K, McClintock SM, McDonald Fischer N, Vora A, Husain MM. Defining treatment-resistant depression: a comprehensive review of the literature. Ann Clin Psych. 2014; 26(3):222±32.
- Tuomilehto J, Lindstrom J, Eriksson J, Valle T, Hamalainen H, Ilanne-Parikka P, Keinanen-Kiukaanniemi S, Laakso M, Louheranta A, Rastas M, Salminen V, Uusitupa M, Finnish Diabetes Prevention Study Group. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med 2001; 344:1343-1350.
- Vormann J, Anke M. Dietary magnesium: supply, requirements and recommendations–results from duplicate and balance studies in man. J Clin Basic Cardiol 2002;5:49–53.
- World Health Organization. Depression fact sheet no. 369 2012 [cited 2016 December 20]. Available from: http://www.who.int/mediacentre/factsheets/fs369/en/.
- Yablon, L.A, Mauskop, A (2011). . Magnesium in headache. In: Vink R, Nechifor M, editors. Magnesium in the Central Nervous System [Internet]. Adelaide (AU): University of Adelaide Press; Available from: https://www.ncbi.nlm.nih.gov/books/NBK507271/
- Yary T, Lehto SM, Tolmunen T, Tuomainen T-P, Kauhanen J, Voutilainen S, et al. Dietary magnesium intake and the incidence of depression: a 20-year follow-up study. J Affect Disord. 2016; 193:94±8. https://doi.org/https://doi.org/10.1016/j.jad.2015.12.056.
